From basics and beyond
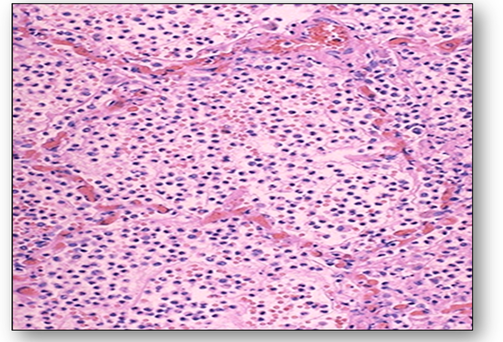
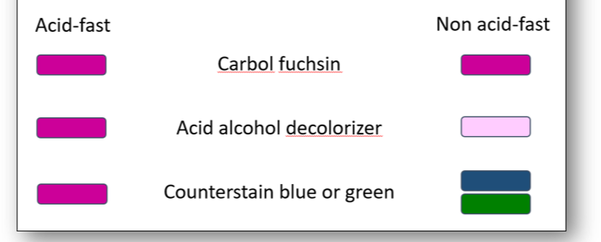
Figure 6. Acid-fast staining
|
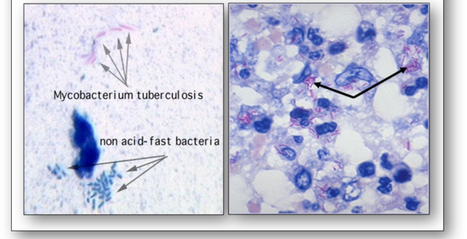
Figure 7. Tubercle bacilli stained with the ZN stain
|
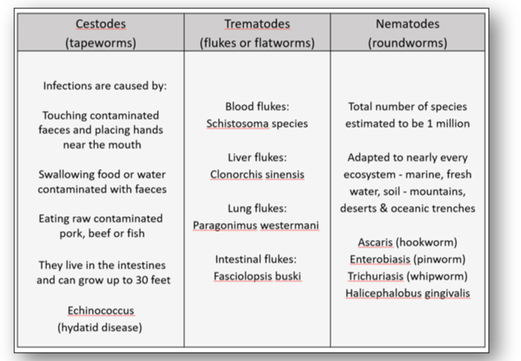
Figure 16a. Classification of helminths
|
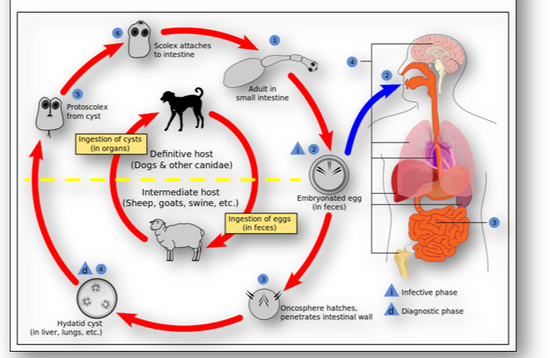
Figure 16b. Life cycle of echinococcus
|
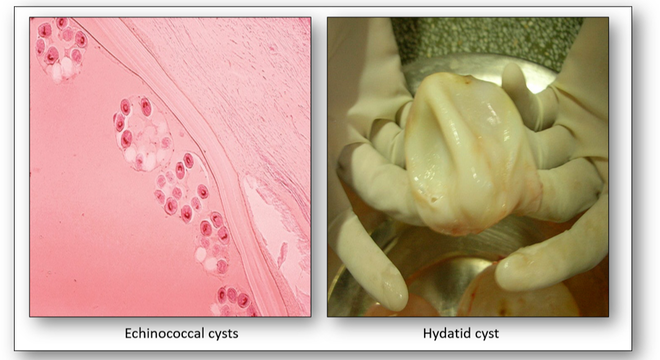
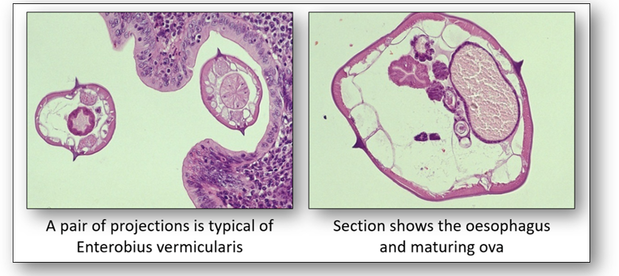
Figure 18. Enterobius vermicularis
|
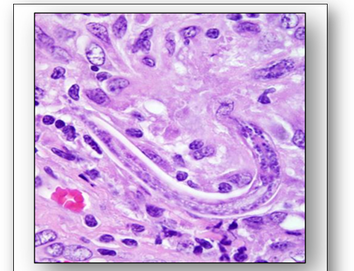
Figure 19. Halicephalobus gingivalis
|

|
The development of cell and tissue growth is complex and is influenced by the combined effect of growth factors, hormones and the availability of nutrients. In disease processes, cells and tissues may go through abnormal changes in size, number and differentiation (Figure 24). For example, high blood pressure will increase the resistance of the heart to blood flow. This increase in functional demand will stimulate both hypertrophy and hyperplasia and result in enlargement of the myocardium (see below).
|
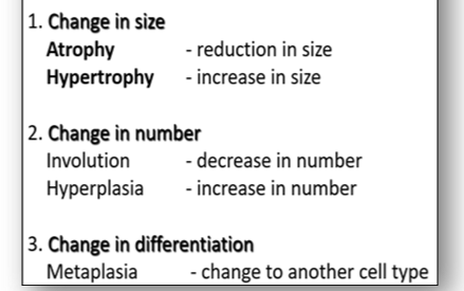
Figure 24. Changes in disease of growth pattern of cells and tissues
|
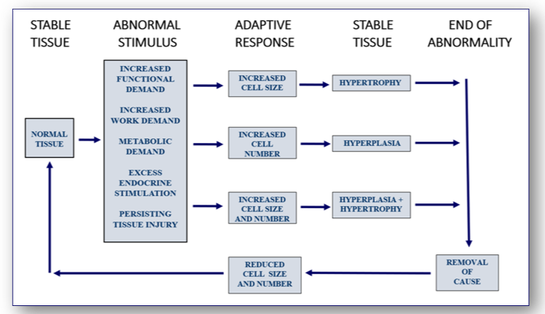
Figure 25. Responses resulting in increased tissue mass
|

Figure 26. Hypertrophy of the left ventricle of the heart
|
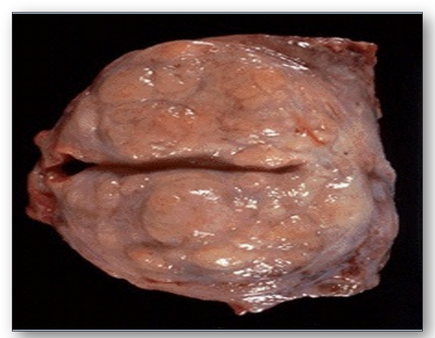
Figure 27. Benign hypertrophy of the prostate
|
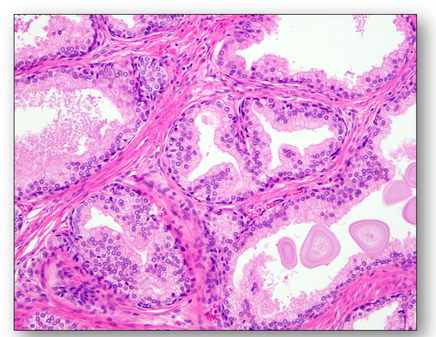
Figure 28. Prostatic hyperplasia showing increased numbers of cells
|
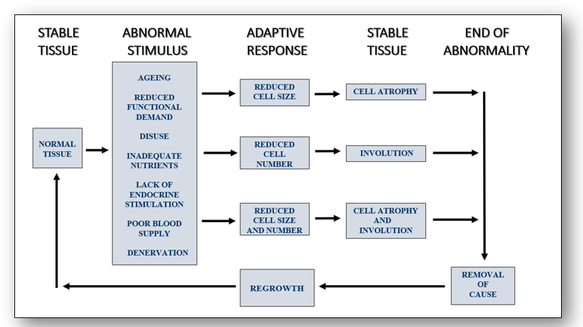
Figure 29. Responses resulting in decreased tissue mass
|
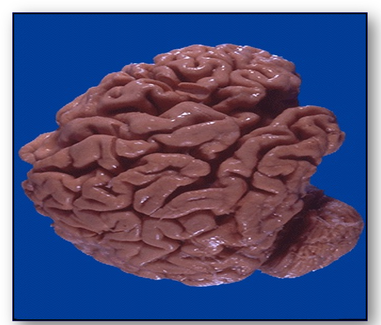
Figure 30. Brain from a patient with Alzheimer's disease
|

Figure 31. Muscle atrophy
|

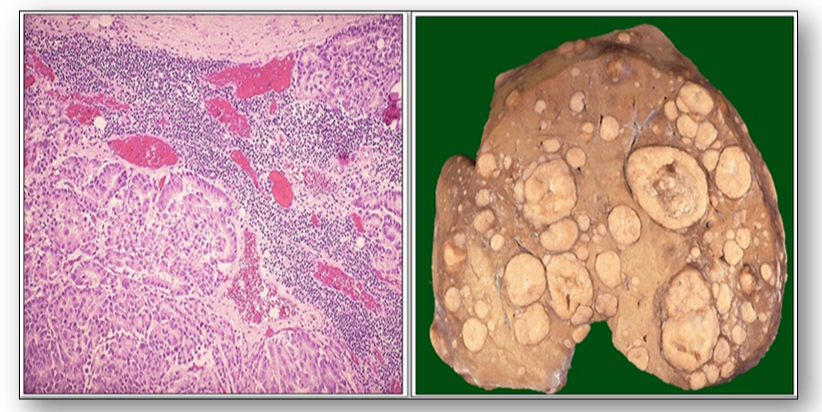
Figure 32. Alcoholic liver changes (see text)
|
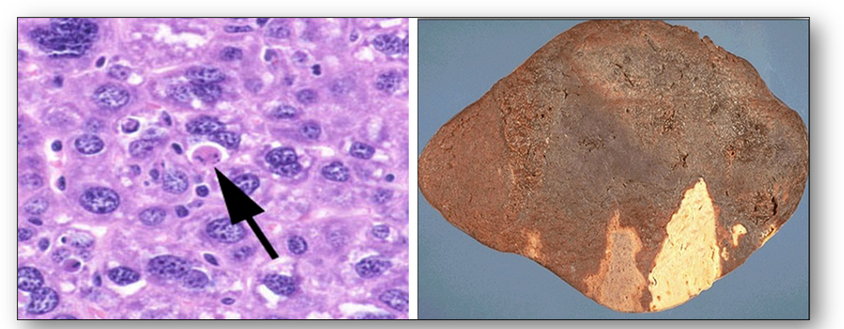
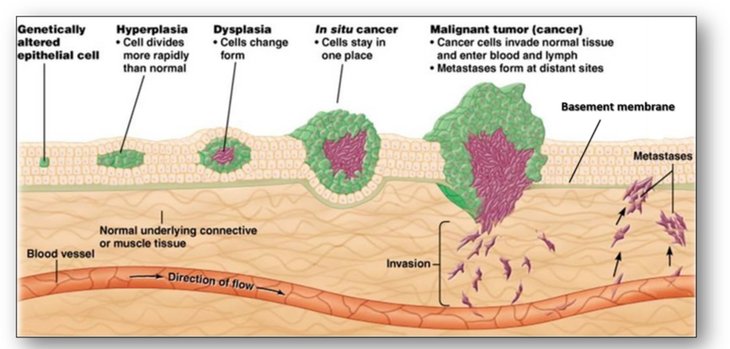
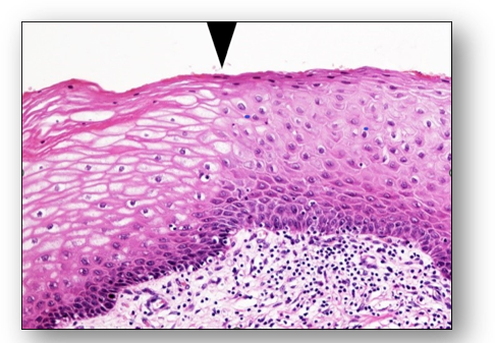
Figure 38. Metaplasia of epithelial cells
|
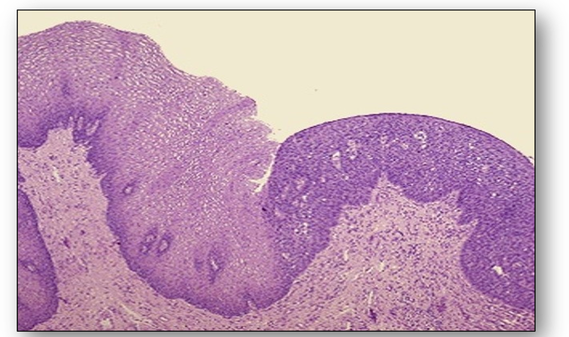
Figure 39. Normal cervical epithelium on the left merging with dysplastic epithelium
|


Figure 47. Benign epithelial tumours showing squamous papilloma of skin (left) and glandular adenoma of bowel (right)

Figure 49. Basal cell carcinoma (left) and a malignant melanoma on the right
|

Figure 48. Malignant epithelial tumours showing squamous carcinoma of skin (left) and adenocarcinoma of bowel (right)
Figure 50. Ductal carcinoma of breast
|
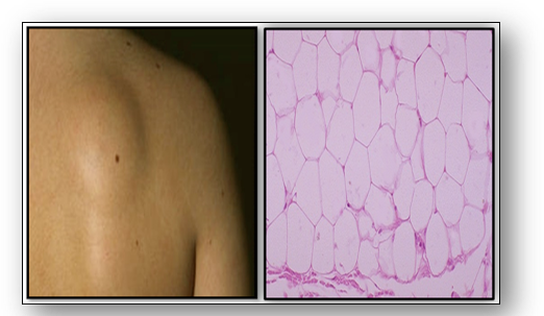
Figure 51. Benign lipoma showing normal adipose tissue
|
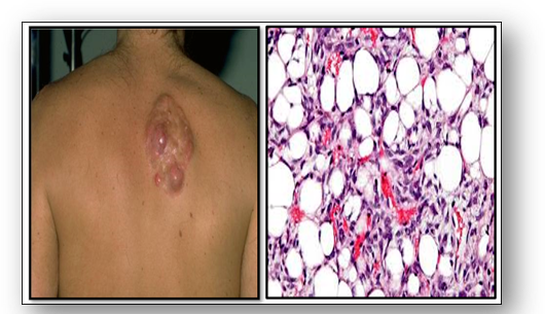
Figure 52. Malignant liposarcoma showing tumour cells in the fat
|
|
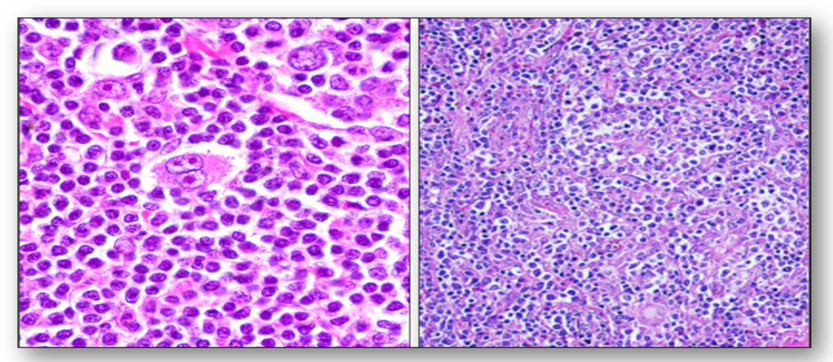
In the nervous system, connective tissue nerve cells are collectively known as glia which are further subdivided into astrocytes, ependymal cells, and oligodendroglia. Tumours arising from glia are termed gliomas and are the most prevalent type of malignant brain tumour in adults (Figure 53). In children, the most common malignant brain tumour is a medulloblastoma, a rapidly growing, nerve cell tumours of the cerebellum, while neuroblastoma, another aggressive malignant tumour develops from immature nerve cells. They are found in several areas of the body and most commonly arises in and around the adrenal glands, which have similar origins to nerve cells. Nerve tumours are abnormal masses that grow on or in peripheral nerves that branch from the brain and spinal cord through the rest of the body. The most common type of benign peripheral nerve tumour in adults is the schwannoma, a tumour of the nerve sheath. Also, ganglioneuromas are rare tumours of ganglion cells and fibres that usually behave as benign tumours. They often start in autonomic nerve cells which manage bodily functions such as blood pressure. |
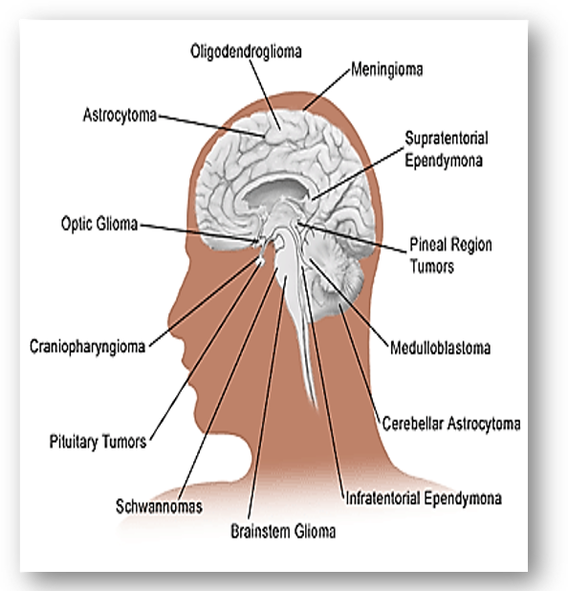
Figure 53. Tumours of the nervous system
|

Mixed tumours are formed by the collision of 2 different tumours that arise together such as adenosquamous carcinoma. Teratomas consist of various tissues, chaotically arranged with no relation to site of origin (see Figure 58a). They are not rare and are usually found in the ovaries and testes. They contain cartilage, bone, epithelia, hair and teeth in the benign form, which appear to be derived from germ cells. Mature teratomas are the most common type of ovarian germ cell tumour. They are non cancerous and often called dermoid cysts (see below). Seminoma is the commonest malignancy of the testis. Of germ cell origin, it is normally found between the ages of 20-50 years. Choriocarcinoma is a highly malignant tumour that originates from trophoblasts. |

Figure 58a. A teratoma containing hair and teeth
|

Figure 58b. Polycystic disease of the kidney
|
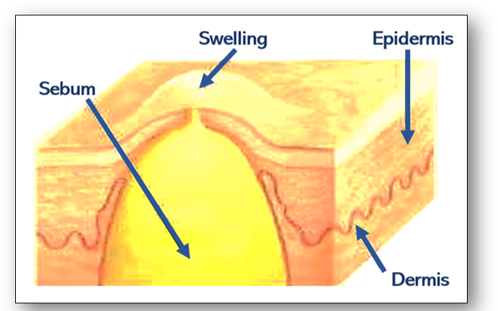
Figure 58c. A sebaceous cyst
|
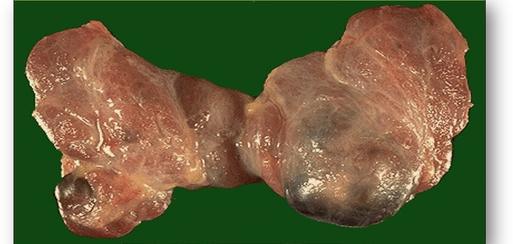
Figure 58d. Distension cysts in a thyroid gland
|
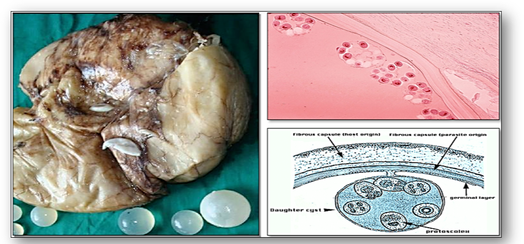
Figure 58e. Hydatid cysts
|
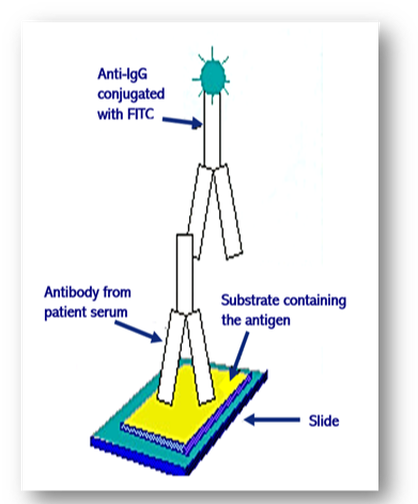
Figure 61. Indirect immunofluorescence
|

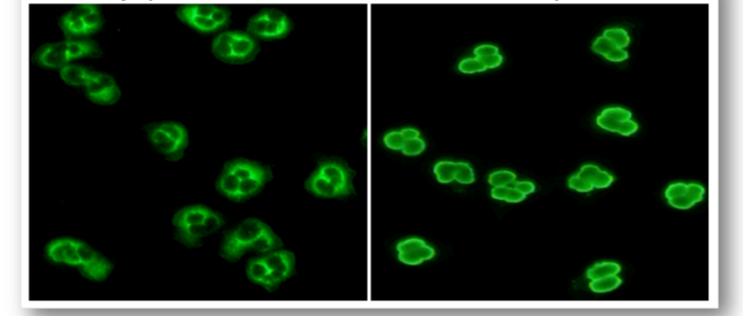
Figure 62. Hep-2 cell and fluorescent staining patterns
|
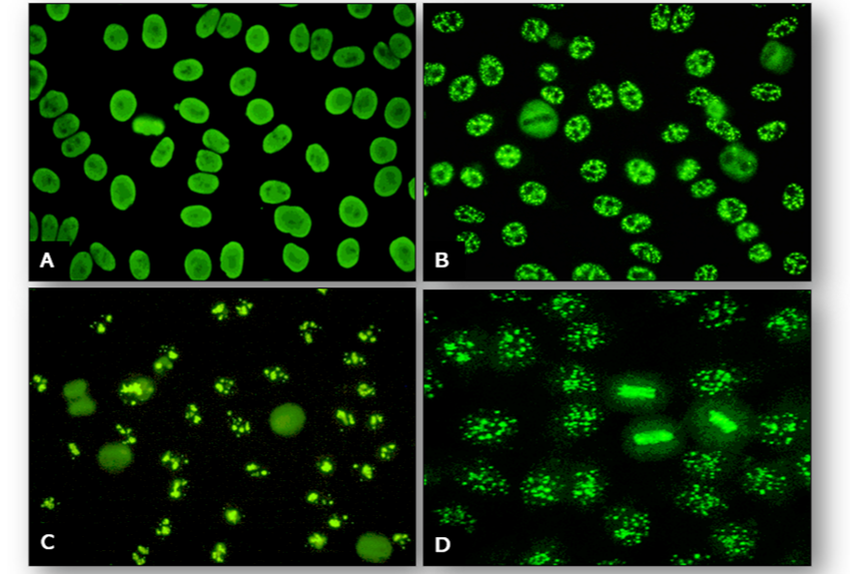
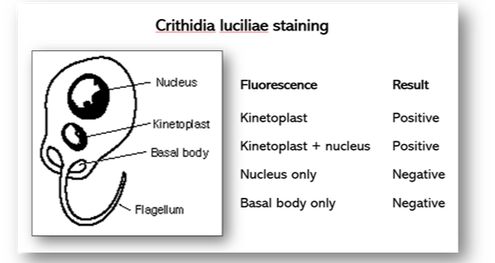
Figure 66a. Crithidia luciliae
|
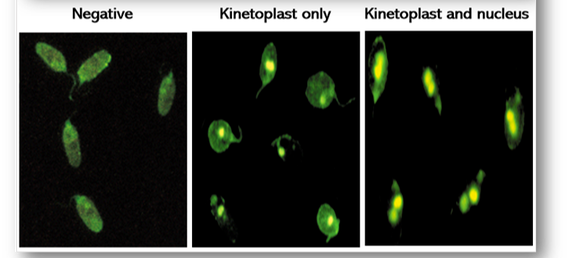
Figure 66b. Staining results for DNA antibodies
|
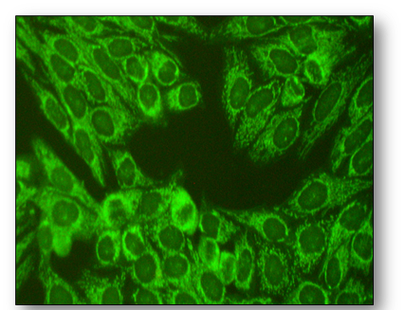
Figure 67. Mitochondrial antibodies in Hep-2 cells
|
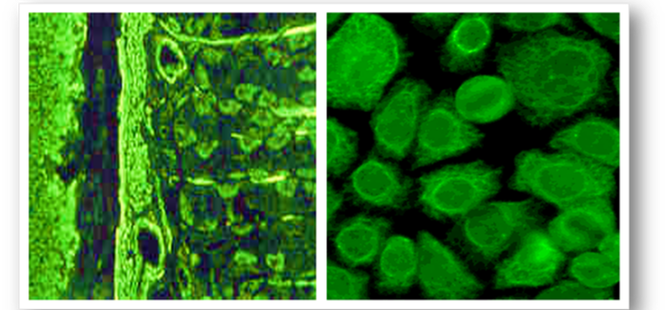
Figure 68. Positive staining for SMA on rodent tissue (left) and Hep-2 cells (right)
|
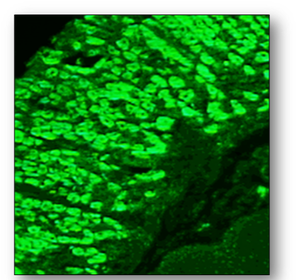
Figure 69. Positive fluorescence in gastric parietal cells
|
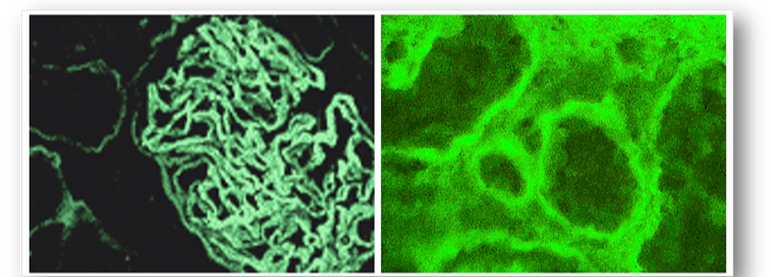
Figure 70. Positive antibodies to GBM (left) and tubular basement membrane (right)
|
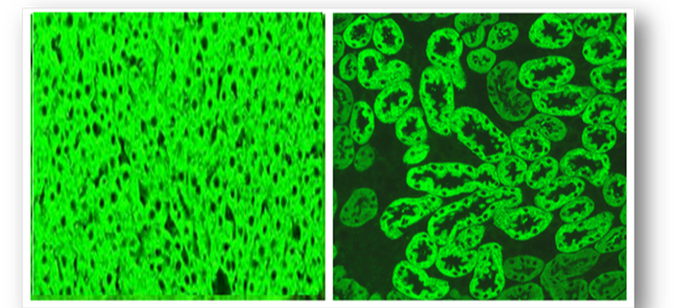

Figure 73. Section of pancreas showing green, fluorescent islet cells
|

Figure 74. Positive endomysial antibodies
|
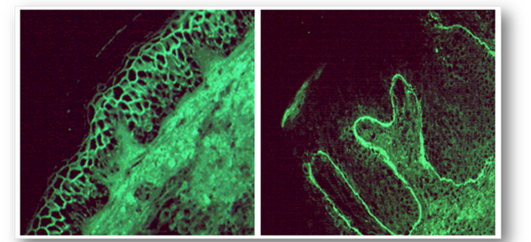
Figure 75. Intercellular fluorescence of pemphigus (left) and linear fluorescence of pemphigoid (right)
|

Figure 76. IgA positivity in the apex of dermal papillae
|

Figure 77. Purkinje cell antibodies
|
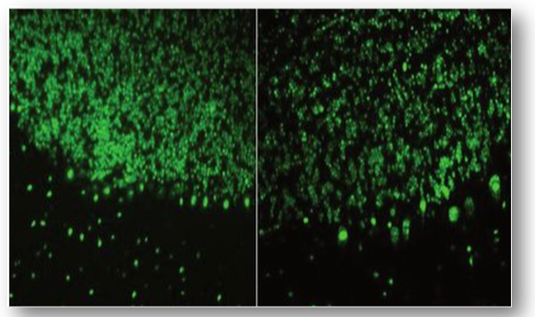
Figure 78. Anti-Hu (left) and anti-Ri antibodies (right)
|